-
 Australia
Australia
-
 Austria
Austria
-
 Belgium
Belgium
-
 Brazil
Brazil
-
 Canada
Canada
-
 China
China
-
 Czech Republic
Czech Republic
-
 Denmark
Denmark
-
 Finland
Finland
-
 France
France
-
 Germany
Germany
-
 Greece
Greece
-
 Hong Kong
Hong Kong
-
 Hungary
Hungary
-
 Iceland
Iceland
-
 India
India
-
 Ireland
Ireland
-
 Israel
Israel
-
 Italy
Italy
-
 Japan
Japan
-
 Korea
Korea
-
 Luxembourg
Luxembourg
-
 Malaysia
Malaysia
-
 Netherlands
Netherlands
-
 New Zealand
New Zealand
-
 Norway
Norway
-
 Poland
Poland
-
 Qatar
Qatar
-
 Romania
Romania
-
 Saudi Arabia
Saudi Arabia
-
 Singapore
Singapore
-
 Spain
Spain
-
 Sweden
Sweden
-
 Switzerland
Switzerland
-
 Taiwan
Taiwan
-
 Turkey
Turkey
-
 United Kingdom
United Kingdom
-
 United States
United States
research use only
CaSR Antibody [A19J6]
Cat.No.: F1579
Application:
Reactivity:
-
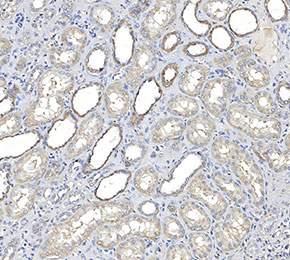 Immunohistochemical analysis of formalin fixed paraffin embedded human kidney tissue with F1579 at 1:100 dilution.
Immunohistochemical analysis of formalin fixed paraffin embedded human kidney tissue with F1579 at 1:100 dilution.
Usage Information
| Dilution |
|---|
|
| Application |
|---|
| IHC, FCM |
| Reactivity |
|---|
| Mouse, Human |
| Source |
|---|
| Mouse Monoclonal Antibody |
| Storage Buffer |
|---|
| PBS, pH 7.2+50% Glycerol+0.05% BSA+0.01% NaN3 |
| Storage (from the date of receipt) |
|---|
| -20°C (avoid freeze-thaw cycles), 2 years |
| Positive Control | Rat brain cerebral cortex tissue; Mouse stomach tissue; Human brain tissue; Human kidney tissue; SH-SY5Y cells |
|---|---|
| Negative Control |
Experimental Methods
| IHC |
|---|
Experimental Protocol:
Deparaffinization/Rehydration
1. Deparaffinize/hydrate sections:
2. Incubate sections in three washes of xylene for 5 min each.
3. Incubate sections in two washes of 100% ethanol for 10 min each.
4. Incubate sections in two washes of 95% ethanol for 10 min each.
5. Wash sections two times in dH2O for 5 min each.
6.Antigen retrieval: For Citrate: Heat slides in a microwave submersed in 1X citrate unmasking solution until boiling is initiated; continue with 10 min at a sub-boiling temperature (95°-98°C). Cool slides on bench top for 30 min.
Staining
1. Wash sections in dH2O three times for 5 min each.
2. Incubate sections in 3% hydrogen peroxide for 10 min.
3. Wash sections in dH2O two times for 5 min each.
4. Wash sections in wash buffer for 5 min.
5. Block each section with 100–400 µl of blocking solution for 1 hr at room temperature.
6. Remove blocking solution and add 100–400 µl primary antibody diluent in to each section. Incubate overnight at 4°C.
7. Remove antibody solution and wash sections with wash buffer three times for 5 min each.
8. Cover section with 1–3 drops HRPas needed. Incubate in a humidified chamber for 30 min at room temperature.
9. Wash sections three times with wash buffer for 5 min each.
10. Add DAB Chromogen Concentrate to DAB Diluent and mix well before use.
11. Apply 100–400 µl DAB to each section and monitor closely. 1–10 min generally provides an acceptable staining intensity.
12. Immerse slides in dH2O.
13. If desired, counterstain sections with hematoxylin.
14. Wash sections in dH2O two times for 5 min each.
15. Dehydrate sections: Incubate sections in 95% ethanol two times for 10 sec each; Repeat in 100% ethanol, incubating sections two times for 10 sec each; Repeat in xylene, incubating sections two times for 10 sec each.
16. Mount sections with coverslips and mounting medium.
|
Biological Description
| Specificity |
|---|
| CaSR Antibody [A19J6] detects endogenous levels of total CaSR protein. |
| Subcellular Location |
|---|
| Cell membrane, Membrane |
| Uniprot ID |
|---|
| P41180 |
| Clone |
|---|
| A19J6 |
| Synonym(s) |
|---|
| GPRC2A; PCAR1; CASR; Extracellular calcium-sensing receptor; CaR; CaSR; hCasR; Parathyroid cell calcium-sensing receptor 1; PCaR1 |
| Background |
|---|
| The calcium-sensing receptor (CaSR) is a class C G protein–coupled receptor that functions as an extracellular calcium sensor, translating changes in ionized calcium concentration into coordinated endocrine and renal responses. It contains a large extracellular Venus flytrap domain that binds calcium and other polycations, a cysteine‑rich region, and a seven‑transmembrane domain that couples predominantly to Gq/11 and Gi/o proteins. Activation of Gq/11 triggers phospholipase Cβ, leading to inositol trisphosphate–mediated calcium mobilization and diacylglycerol–dependent activation of protein kinase C, while Gi/o coupling suppresses adenylate cyclase and lowers cAMP levels. In parathyroid chief cells, increased extracellular calcium engages CaSR to inhibit parathyroid hormone (PTH) secretion and promote PTH internalization, establishing a major negative feedback loop for systemic calcium homeostasis. In the kidney, CaSR signaling in the thick ascending limb and collecting duct influences calcium and magnesium reabsorption, phosphate handling, and urine concentration by interacting with transporters such as NKCC2, ROMK, and ENaC, and by intersecting with MAPK and mTOR pathways that modulate cell growth and tubular function. CaSR‑dependent signaling also contributes to regulation of vitamin D metabolism and bone turnover through its effects on PTH and downstream endocrine axes. Germline loss‑of‑function mutations in CaSR cause familial hypocalciuric hypercalcemia and neonatal severe hyperparathyroidism, characterized by elevated serum calcium and inappropriately normal or high PTH, whereas gain‑of‑function mutations lead to autosomal dominant hypocalcemia with low calcium and suppressed PTH. |
| References |
|---|
|
Tech Support
Tel: +1-832-582-8158 Ext:3
If you have any other enquiries, please leave a message.
Products are for research use only. Not for human use. We do not sell to patients.
©Copyright 2013 Selleck Chemicals. All Rights Reserved.